Anemia: Iron deficiency or just inflammation?
In this article, we will explore the topic of anemia, essentially what most would call iron deficiency. We will also dive into the more complex and nuanced connection to metabolic health issues or cellular inflammation, which can present and cause anemia of inflammation.

Iron is a key heavy metal used by every cell in our bodies for various purposes. Iron serves a role in mitochondrial iron-sulfur clusters that help transfer electrons so we can make energy!
Our body has around 3.7 grams of iron acquired from diet—alone and with a more complex regulatory and excretory system. About 75% of that is utilized inside the hemoglobin in our blood, which assists in transporting oxygen around the body for energy production. The remaining is found in myoglobin, and around 1 gram is stored inside ferritin to fulfill future needs.
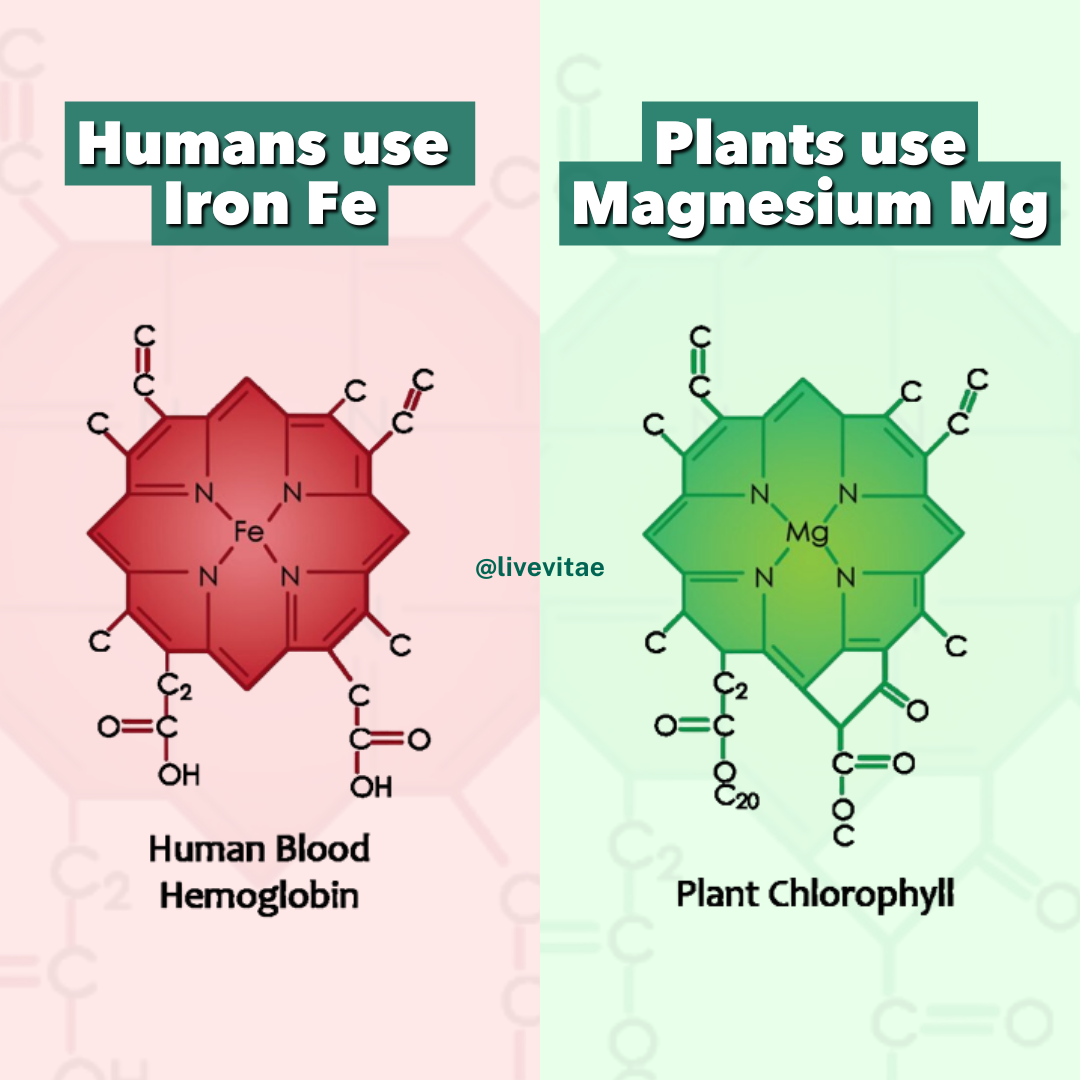
Iron is the center atom used to make porphyrin, a key molecule in getting oxygen transported around our bodies, holding and transferring electrons in mitochondria, and even serving as the building block for vitamin B12.
Animals uniquely conserve iron, while plants are preserved for magnesium. Iron has MORE electrons, which can be excited by the power of light, water, and magnetism.
Iron: too much or too little?
Despite this and the massive utility of iron in maintaining and optimizing health, it is relatively easy to get an excess of iron, and it becomes especially detrimental when that excess iron is not bound. Iron requires proteins and compounds (like porphyrin shown in the image above) to secure it so it can be used effectively and correctly.
Think of it another way: our cells can’t use free unbound iron. Our cells store free, unbound iron and complex it with proteins to make it usable in the first place.
A perfect example of a protein that requires iron as part of it, is hemoglobin. That’s your oxygen-carrying protein; without the iron, it could not carry oxygen to cells. It also relates to heme synthesis, which is controlled and started in the mitochondria. Making mitochondria health key to the feedback that loops to optimizing health. Heme synthesis requires several steps and nutrients to work. Iron, copper, vitamin C, vitamin B2, vitamin B6, vitamin B9, vitamin B12, glycine, vitamin A, and B1.
“The incorporation of radioactive glycine and δ-aminolevulinic acid into heme in vitro was decreased in vitamin B6 , niacin, pantothenic acid, riboflavin, and thiamine deficiencies, and this became more pronounced with the duration of the deficiencies.” 1
However, if iron is found outside the protein, some potentially unwanted circumstances can occur.

Iron overload and dysregulation
Iron can be found outside in its free form in many conditions and contributes to worsening health states.
However, the degree to which iron is found hanging freely can be different if we consider iron dysregulation versus iron overload. The means of measuring this with tests is not absolute.
Iron dysregulation is far more common, and even being infected with the common cold can cause iron dysregulation. When iron dysregulation is present, the general features of iron uptake and transport are affected. One of the markers that will increase with this is ferritin. However, iron levels in tissues may remain completely unaffected. This is because the body is making sure to keep iron stored so as not to worsen health. The image below shows the differences in what it can look like between the two states, which might not apply in all cases.

What happens when there is inflammation?
A clear example is the setting of acute and adaptive inflammation (an acute phase response), in which we would see changes in the blood with ferritin, iron, and ceruloplasmin. This safeguards iron—to protect the host from further damage and inflammation—from self, viruses, and bacteria requiring iron for their metabolism. “Iron is like chocolate to bacteria.” 1
You do not want iron to be free and unprotected. Instead, we see feedback loops of shutting down iron physiology, which has multiple downstream effects with heme synthesis, energy production, free radical signaling, thyroid hormone production, dopamine production, and everything else associated with iron.

We lock this iron inside our cells—tissues to protect us in the short term. The issue is the aftermath: what happens when we can not respond or get out of this mayday inflammatory signal state?
We continue to lock up iron and make it unavailable, which creates downstream effects such as metabolic imbalances, hormonal problems, and “iron deficiencies” from lack of utilization.
Iron dysregulation and neurodegeneration?
It can get pretty serious, though. For example, iron dysregulation is a feature of neurodegenerative disorders. At first, there is iron dysregulation in neurodegenerative diseases. Then, if it continues, iron overload can occur and cause a type of cell suicide called ferroptosis. 11
Ferroptosis is a suitable marker when doing in vitro work to determine if an excess of iron is stored within cells and tissues. 12 Even if iron were to be chelated, there would be a residual effect on the cells that would reduce their ability to stay redox active. Making the prevention of iron accumulation key.
“Three essential hallmarks define ferroptosis, namely: the loss of lipid peroxide repair capacity by the phospholipid hydroperoxidase GPX4, the availability of redox-active iron, and oxidation of polyunsaturated fatty acid (PUFA)-containing phospholipids.” 3

What causes iron overload?
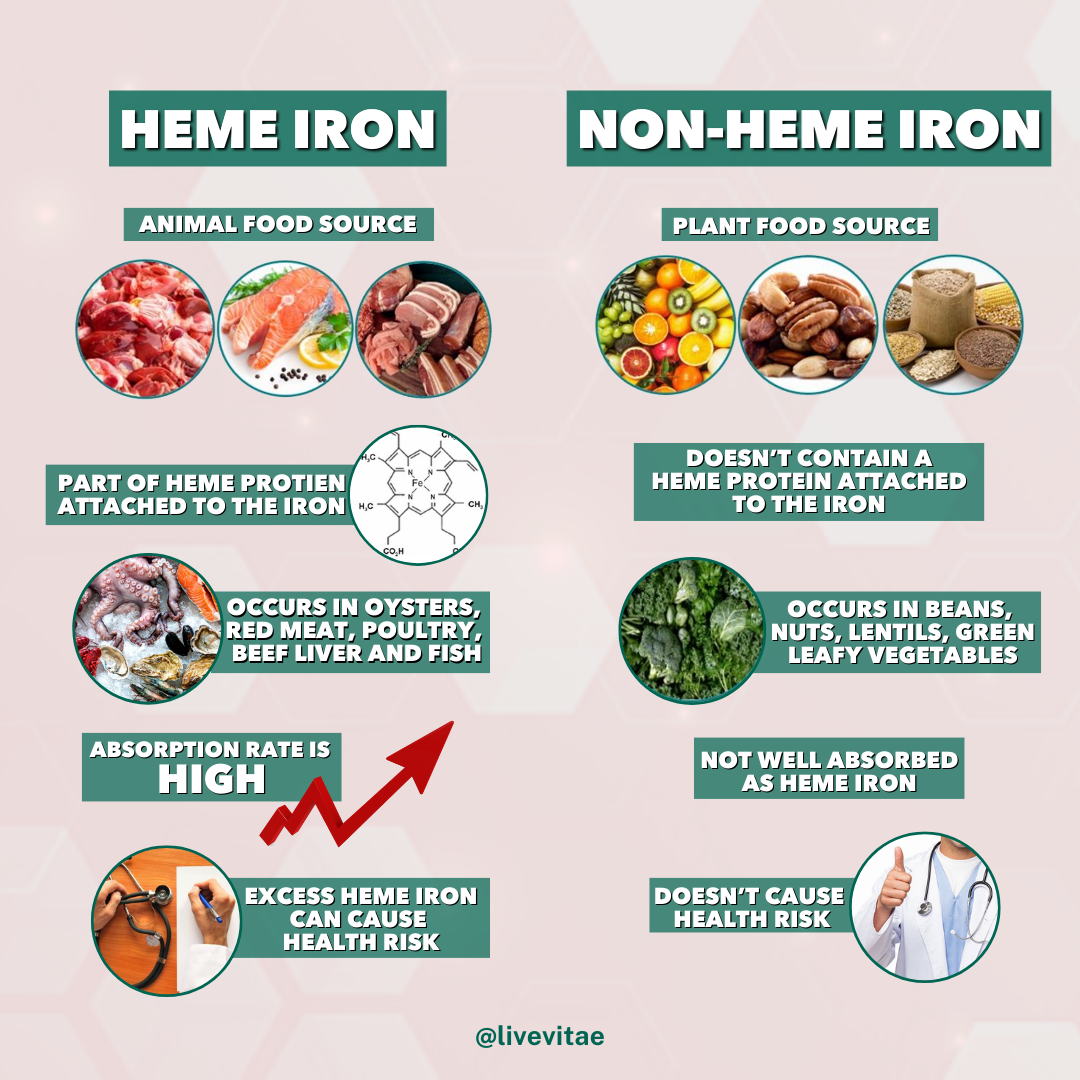
Potentially, too much iron can come from the diet. This is typically a consortium of too much heme iron from animal foods and the lack of plant foods, specifically tannins, oxalates, polyphenols, and phytic acid, that have a partial chelating effect. Those on a strict carnivore or heavy animal-based diet without plants can easily accumulate iron. Additionally, those diets abundant in iron but lacking copper, vitamin A, and zinc also run the risk of transport and utilization issues.
No nutrient works independently in the human body.
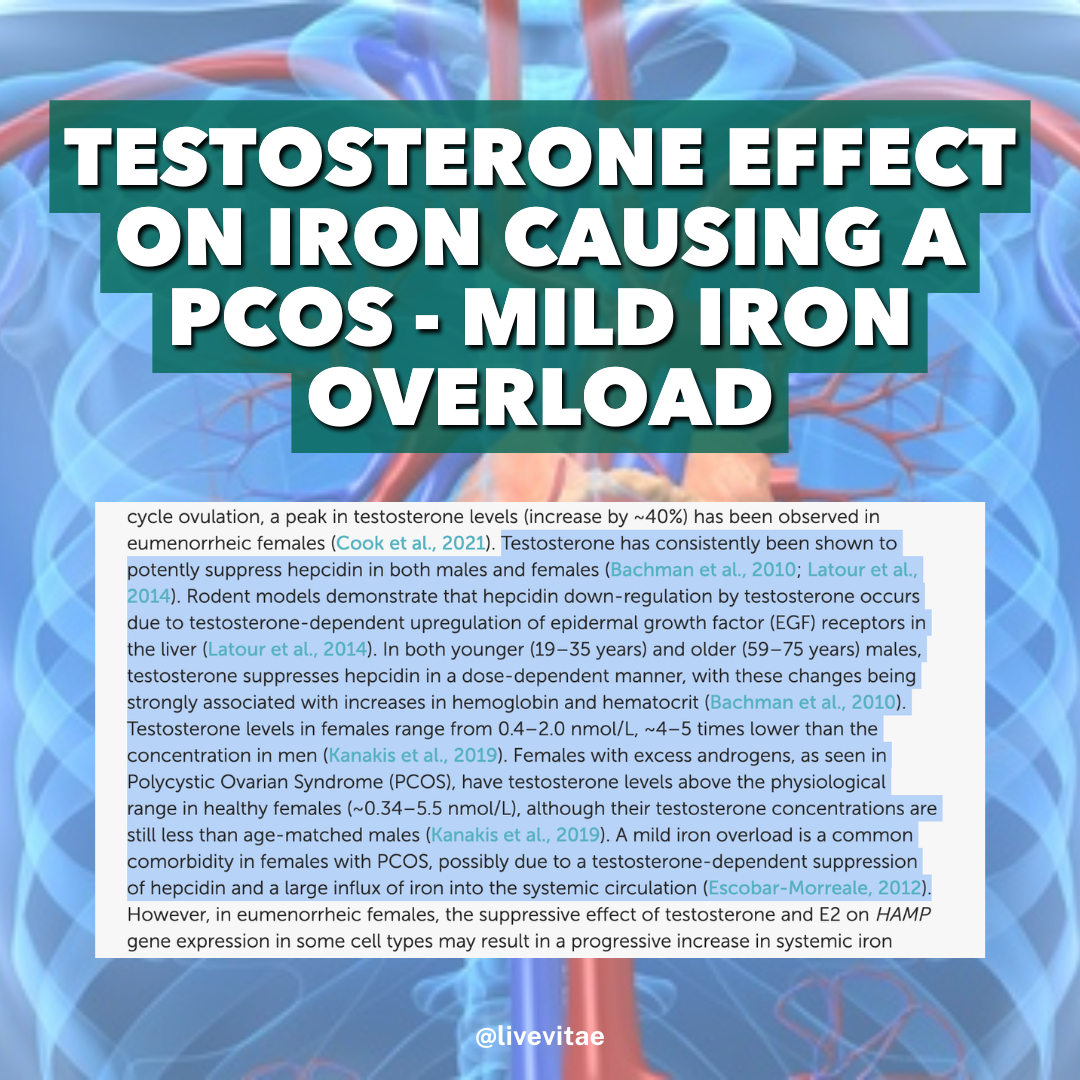
Secondly, if the hormone hepcidin is not produced adequately or signaled via the gut, interestingly, vitamin C deficiency becomes common 7. Without adequate vitamin C, glutathione production drops. It makes the body very sensitive to oxidation. This, coupled with excess iron being already reactive, causes redox dysregulation. Theoretically, the vitamin C deficiency could also be because the more vitamin C there is, the more iron can be used. It may serve as a protective mechanism by the body.

The gut and iron connection
Inflammatory signals in the gut, gut dysbiosis (use of antibiotics or small intestine overgrowth, viral burden, and parasites all likely influence cytokine signaling, which regulates how the liver senses our health, which influences how much and when to make hepcidin to control iron absorption.
“Hepcidin deficiency causes iron overload in hemochromatosis and anemias with ineffective erythropoiesis. Hepcidin excess causes iron-restrictive anemias including anemia of inflammation. The development of hepcidin diagnostics and therapeutic agonists and antagonists should improve the treatment of iron disorders” 4
Excess inflammatory signals are known to increase interleukin 6, which has knock-on effects with hepcidin production, altering fundamental dynamics of how iron is regulated with absorption in the gut, in macrophages in the spleen, in the bone marrow, and transportation with how ferroportin works inside cells.
Iron uptake via digestion is typically also reduced, thanks to normal hepcidin production. Generally, hepcidin signaling is impaired in genetic cases of hemochromatosis. In such circumstances when we take up too much iron, the body protects us from taking up any more by increasing the amount of hepcidin secreted by the liver. Hepcidin can also be increased during inflammatory events, whether because of iron or other factors. 13
Iron excess and diet
Generally, iron requirements are pretty low compared to other vital nutrients like calcium. Men need about 8-12 mg of iron daily, and women need about 12-18 mg daily. That need increases if the woman is premenopausal due to blood loss during menstruation or pregnancy.
Many diets differ in the amount of bioavailable iron they provide. Plant-based diets see most of the iron in the form of non-heme iron. This is the type of iron that’s not bound to heme protein. This type of iron is generally lower in bioavailability. This appears more so because many plant-based foods contain iron absorption inhibitors like phytic acid.
Conversely, because plant-based diets contain more vitamin C, more iron could be absorbed. Combining greens and meat offers an effective way to really increase iron uptake in the gut. However, limiting calcium intake in these meals can be helpful.

Iron mediated inflammation
Iron is a very reactive metal, mainly because of its missing electrons. Metals with an unfilled number of electrons will seek to take it from other sources. This means it will react if your cells, proteins, and lipids are exposed to free, unbound iron. This is normal and how our metabolism works (free radicals are not always harmful). We use oxygen and iron, two of the most reactive elements known.
When it does, the type of reactions iron catalyzes is destructive. The same is true for copper, which MOST people forget about. These two metals are called transitional metals—they are very unique.
A perfect representation of this is when immune cells come into contact with free iron, or mitochondria come into contact with free iron. In both cases, mitochondria and immune cells experience a reaction known as the Fenton reaction. 14

The Fenton reaction types (image shown above 6), is demonstrating that iron ions will react with water, hydrogen peroxide, or hydroxyl radicals formed from either water or hydrogen peroxide. When it does, the iron becomes stripped of an electron and will seek to regain it by reacting with nearby molecules like lipids. This can cause lipid peroxidation in return.
In the Fenton reaction, iron essentially oxidizes water, superoxide (generated as a byproduct of metabolism), or hydrogen peroxide (which our immune cells make to kill off microbes). The reaction is vigorous and damages nearby components of cells. Thus triggering the inflammatory cascade.
We have an antioxidant backup system to handle this in small doses or critical, specific, demanding times; however, no lingering “turning down” signal can become drained when our health becomes imbalanced.
Now, suppose we scale this at a tissue level. In that case, we can see why conditions like low ferritin but high iron, low transferrin concentration, iron overload, and hemochromatosis are all significant concerns. In all of these conditions, you essentially have a large amount of unbound iron and simply insufficient proteins to capture and transfer this iron safely.

The image above highlights iron metabolism within the body as a whole. 7
Iron is taken up within the intestines with contributing factors and proteins to load onto transferrin.
Transferrin carries iron throughout the body to involve it in normal cellular functions. What doesn’t get used undergoes breakdown and turnover by immune cells.
Iron and ferritin
The most important protein in the body involved in normal iron metabolism is ferritin. Without ferritin, iron would not have a means of being stored safely within cells. That is the sole purpose of ferritin. It is the storage marker of iron, so most conventional doctors use it as a proxy for iron.
Ferritin can exist in two forms: an iron-empty form and one that already has iron inside. Even mitochondria have their type of ferritin, known as mitochondrial ferritin.
Below is an in-silico remodel of ferritin's appearance from the outside (top) and a cross-section (bottom). The center is where iron is stored. 8

Iron and ferritin key point
When the body has excess free iron, ferritin will be sent out to scout around and scoop up any excess free iron. In the scenario where the free iron is already causing havoc and damaging tissues by the reactions described above, ferritin will seriously increase to stop any further damage.
This is why ferritin is known as an acute response protein. It responds to free iron and since unbound iron causes inflammation, ferritin being high is a sign of that inflammation.
However, here is where the confusion sets in with iron deficiency anemia.

Iron deficiency anemia—real or not?
A recent change in the perception of what defines iron deficiency anemia has occurred. This is because most tests that determine iron deficiency consider blood concentrations of iron. 15 This is not always a good representation of iron status in individuals, as iron is mainly concentrated within tissues.
This has caused a division between people who view iron deficiency anemia as an accurate diagnosis when blood levels of iron are low and people who view blood levels of iron as distracting since a majority of iron will be within tissues. The reality is both camps can be right in the proper context, and what they have not considered is the highly complex metabolism of iron. 15
Iron deficiency anemia is a genuine condition and is present primarily in women. Why?

The main reason is because of the loss of blood during menstruation. Potentially, you could add the push towards more plant-based diets, increases in phytic acid, and lower vitamin C intake plus modern stressors impacting digestion such as stomach acid production, all hindering iron absorption.
Men do not lose blood as quickly, and iron is not excreted so easily either with more risk of iron overload later in life.

However, iron overload in tissues, with specific accumulation in certain tissues as we age, is also true. Many of these iron overload situations are due to unique gene inheritance that contributes to too good an ability to absorb iron. 16
For example, a gene variant that allows iron to cross from the intestine into the bloodstream is overactive in specific individuals with hemochromatosis type IV. In this case, the liver hormone hepcidin, which stops iron uptake when there’s an excess, is not affecting the gene as it should. So, the body continues to take in more and more iron.
Contextualizing is vital as many individuals have mixed genes for iron absorption, storage, and transporter proteins.
Gut dysbiosis causes iron deficiency.
Iron deficiency also occurs in the case of microbial interaction. We have to remember that iron is equally as important for microbes as it is for us.
Generally, microbes will use iron for their own purposes when they sense something is off in the body. This tends to come from the production of pro-inflammatory cytokines, such as IL-1 and IL-6. 17
This is why hepcidin gets produced in return, to prevent the microbes from using iron for their own purposes and prevent excess free iron in the body. The foods we eat can also alter the gut pH and increase the amount of iron available for microbes to use. One example of this is with high-fiber diets that allow the bacteria to ferment the fiber. When they do, short-chain fatty acids that are slightly acidic are produced, helping make iron more bioavailable for them.

Optimal Health = Mitochondria + Iron Regulation
In most individuals, iron overload is rarely the problem. We live in a world that is bombarded by substances and compounds that are able to chelate iron and reduce its availability, even more so in females.
Coffee, smoking, medications, tea, heavy metals that compete and strip iron, stress that increases the turnover rate of iron, and many more compounds strongly reduce the amount of iron available for our cells to use. Further, our general health is a tremendously important factor in determining if our cells will use iron properly or not.
Energy + Order = Optimal Health
When there are disturbances, like metabolic dysregulation, in our metals and electrolytes, this can be the result of multiple factors such as pathogens, circadian rhythm, pH, sleep apnea, and much more such as mercuri’s effect on zinc, which disturbs iron.

Why I don’t recommend hair mineral testing
The mineral balancing community gets fixated on hair testing and selling supplements where the mechanisms discussed above can easily alter what is excreted in hair and truly happening inside the cell. I think using hair testing alongside over-tests can be more useful, but I find this community very narrow-minded.
What is the best way to test iron?
It is not with hair mineral testing but it is using the gold standard method, which is blood testing. This would ideally be done fast and in the morning using not just iron as a marker but a collection of markers, which I have detailed below.

Factors causing iron dysregulation
Being overweight and obese already creates a dilemma in which fat cells begin to experience inflammation (by releasing proinflammatory adipokines; these are cytokines specific to fat cells), and a consequence of this is that iron gets liberated in addition to endotoxins, estrogens and altered leptin sensitivity in the hypothalamus—worsening the inflammatory response.
An unhealthy body due to the presence of far too much lipid peroxidation is likely to experience ferroptosis more often than someone who is healthy, redox stable, and has low oxidative stress. 18
Since the main use of iron comes down to mitochondrial respiration, their health can determine the health of the cells they reside in and as a collective, the health of the organism; us. In turn, this affects how we metabolize and utilize iron. Either contributing to inflammation or to homeostasis.

Circadian rhythm disruption alters iron regulation in many ways from digestion, to mitochondria function to regulatory transcription factors and transporters. Aligning your circadian rhythm is one of the most fundamental aspects to optimal health, yet our modern environment alters this.
Energy deficiency, aka Relative Energy Deficiency Syndrome (REDS). This is more pronounced in females who are training intensively. This is when iron can be lost through the action of running, foot striking, or physical activity. Further compounded by the lack of energy consumed to offset the expenditure, it creates a calorie deficit influencing thyroid hormone regulation with transporters, slowing down metabolism systemically with leptin and estrogen signalling disturbed, alteration with iron absorption and loss = inducing menstruation issues such as amenorrhea. 10
Important iron functions in the body
Aside from its roles in energy, metabolism, and oxygenation, iron plays a critical role in detoxification. The main enzymes that our bodies use to break down exogenous compounds and aid in detoxification are reliant on iron.
Specifically, the cytochrome enzymes, otherwise known as CYP enzymes. The iron atom sits inside the center of these enzymes, where the reactions occur. Iron’s role in these enzymes in particular is to produce water to help make exogenous compounds more water soluble.
Without it, the body could not get rid of the compounds and toxicity of substances would quickly accumulate.

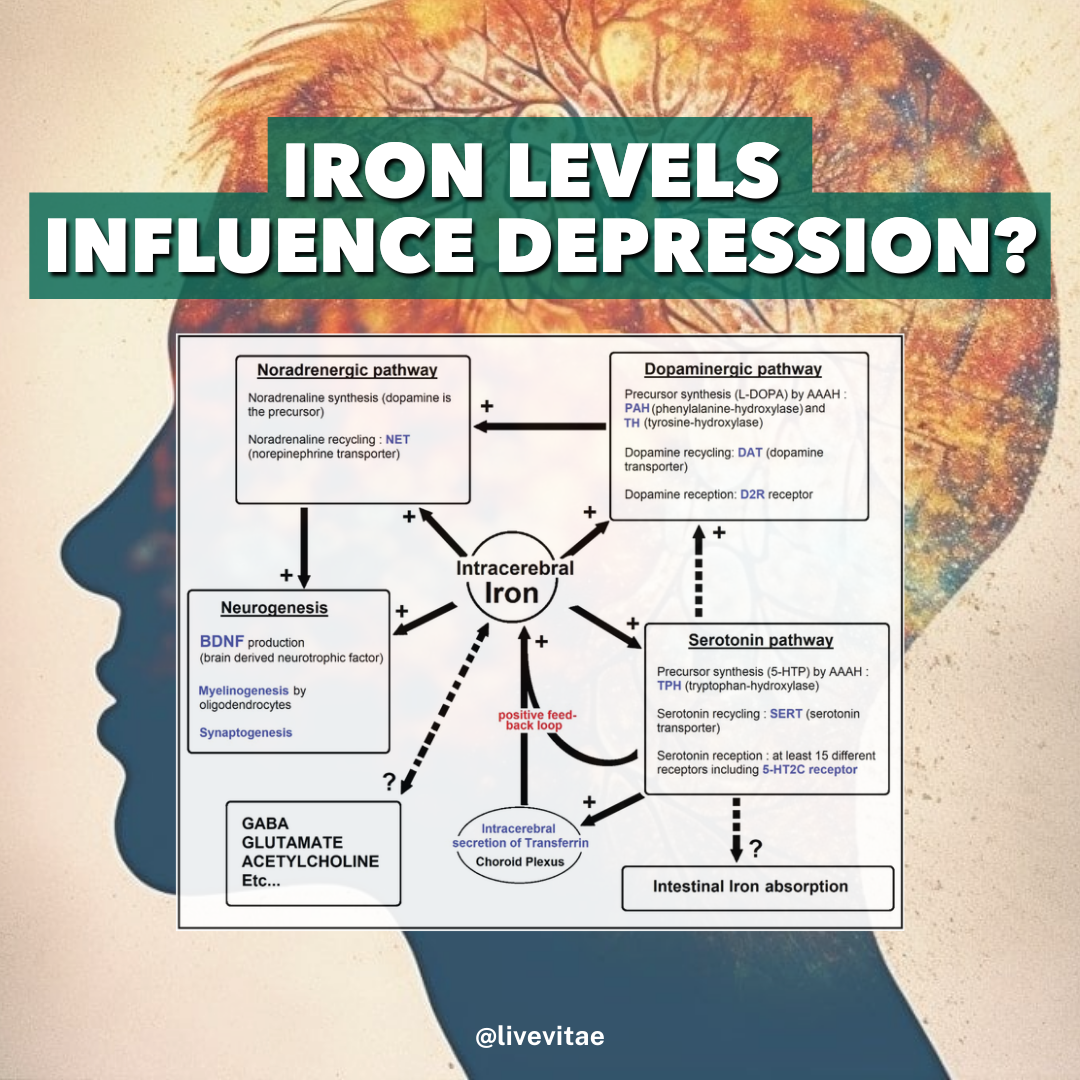
Iron regulates dopamine and thyroid hormones
Iron is a critical cofactor in the production of dopamine through its enzyme tyrosine hydroxylase and also the production of dopamine receptors. In fact, the areas of the brain associated with the highest dopamine production such as the substantia nigra, contain a large amount of iron. Iron excess and dysregulation can also contribute to neurodegenerative diseases like Parkinson’s. 19
So there is a fine relationship between available iron for needed reactions to either produce dopamine and its receptors, or dysregulated iron metabolism causing the accumulation of metabolites like neuromelanin. 20
Similarly, iron is also critical for thyroid function. In an experiment done on rats, the rodent was depleted of iron at severe levels drops, T3 levels and norepinephrine markedly. When iron was repleted there was normalization of T3 production in the rats within seven days. 21 Additional studies on humans consistently show iron deficiency anemia (true iron deficiency) cause lower T4 and T3 levels.

How to resolve iron imbalances?
Iron imbalances and iron dysregulation require in depth examination as there are a large number of potential contributing factors. This is the key issue with modern medicine and functional medicine alike.
Modern medicine does not yet translate research done on iron dysregulation into clinical settings. One is often assessed for a handful of iron markers like transferrin, ferritin, and total iron binding capacity. Though these markers are not correlated with changes in tissue and metabolic function outside of simply iron.
For example, it’s well documented that increases in ferritin indicating inflammation may be totally separate from iron stores. One could be deficient in iron, but have elevated ferritin, because of inflammation from adipose tissue. 22
To resolve iron imbalances, testing for iron markers is the first step. Taking into account:
TIBC
UIBC
Ferritin
Soluble transferrin receptors (more advanced)
Transferrin percent saturation
Red blood cell count
MCV
MCH
MCHC
Hematocrit
Together, these markers can explain how well the cells are using iron, if there is true anemia, or if there is an iron imbalance. Then one would need to take account of health history and potential factors influencing iron metabolism. This is where going deeper with a practitioner is required.
Additionally, looking at dopamine and noradrenaline metabolites on the organic acid test, or cerruplasmin, copper, and zinc in a more ellbaorate blood test could expose potential interactions. Personally, I find that hair tissue mineral analysis testing is not the best assessment tool to utilise, but can be handy if budget testing scenarios are limited.
Assessing for other metals that can compete with and displace iron such as lead, is an overlooked part of iron dysregulation. Excess use of zinc can complicate iron absorption and utilization. The type of diet one consumes also affects iron absorption as mentioned previously.
Iron is not the only nutrient the body needs to function properly. Iron works in conjunction with many other micronutrients and vitamins. For example, foods that contain large amounts of iron also typically contain copper. Copper and iron are both required for mitochondrial respiration to occur.
Donating blood and consuming copper rich foods as is done in the root cause protocol can quickly lead to low stores of iron within ferritin and reduce mitochondrial function, oxygenation of tissues, and increase uptake of unwanted heavy metals like cadmium.
The interplay between nutrients, the type of diet one consumes, the daily lifestyle practices one attentively or inadvertently does, all affect iron homeostasis and health.
Wrapping up iron dysregulation
The multi-system role of iron makes it an incredibly important micronutrient for general health. The way the body handles iron can be tricky. Our personal genotype, our food, lifestyle choices, and our environments, all play a role in how iron gets used by cells.
When things go awry, such as in the case of inflammatory conditions, low redox potential, mitochondrial dysfunction, iron markers like ferritin can increase, while iron use itself decreases. Making the body appear as if it has adequate iron due to tissue stores, but it’s not properly utilizing it.
Certain factors like the gut microbiome and infectious agents can also disrupt normal iron metabolism because of their preference for the metal. In these scenarios, iron deficiency is a common misdiagnosis and patients believe they require further iron supplementation to see improvements.
While it can help for some, it can worsen the situation for others. Without addressing the root causes, iron supplementation acts only as a bandaid.
Iron deficiency is, however, a true concern, and especially more so for women. It is ironic that women suffer the most from hypothyroidism and iron plays an integral role in thyroid hormone production.
Likewise in males, dopamine deficits and dopaminergic changes are very common due to modern lifestyles. Iron is known to play a role in both the creation of dopamine and the response to dopamine by its cognate receptors.
This makes addressing iron through nutritional, lifestyle, and interventional methods critical for optimizing health.

WORK WITH a health practitioner who can connect the dots, with context and show you how to apply these practices in the real world.
REFERENCES:
Richert, D.A. and Schulin, M.P. (1959) ‘Vitamin interrelationships in heme synthesis’, The American Journal of Clinical Nutrition, 7(4), pp. 416–425. doi:10.1093/ajcn/7.4.416.
Richert, D.A. and Schulin, M.P. (1959) ‘Vitamin interrelationships in heme synthesis’, The American Journal of Clinical Nutrition, 7(4), pp. 416–425. doi:10.1093/ajcn/7.4.416.
Dixon, S.J. and Stockwell, B.R. (2019) ‘The hallmarks of ferroptosis’, Annual Review of Cancer Biology, 3(1), pp. 35–54. doi:10.1146/annurev-cancerbio-030518-055844.
Nemeth, E. and Ganz, T. (2023) ‘Hepcidin and iron in health and disease’, Annual Review of Medicine, 74(1), pp. 261–277. doi:10.1146/annurev-med-043021-032816.
Ganz, T. (2019) ‘Anemia of inflammation’, New England Journal of Medicine, 381(12), pp. 1148–1157. doi:10.1056/nejmra1804281.
Hatipoğlu, G. and Mahindaratne, M. (1964) What is the actual mechanism of Fenton reaction?, Chemistry Stack Exchange. Available at: https://chemistry.stackexchange.com/questions/95227/what-is-the-actual-mechanism-of-fenton-reaction
Camaschella, C., Nai, A. and Silvestri, L. (2020) ‘Iron metabolism and iron disorders revisited in the hepcidin era’, Haematologica, 105(2), pp. 260–272. doi:10.3324/haematol.2019.232124.
Richert, D.A. and Schulin, M.P. (1959) ‘Vitamin interrelationships in heme synthesis’, The American Journal of Clinical Nutrition, 7(4), pp. 416–425. doi:10.1093/ajcn/7.4.416.
Richert, D.A. and Schulin, M.P. (1959) ‘Vitamin interrelationships in heme synthesis’, The American Journal of Clinical Nutrition, 7(4), pp. 416–425.
Richert, D.A. and Schulin, M.P. (1959) ‘Vitamin interrelationships in heme synthesis’, The American Journal of Clinical Nutrition, 7(4), pp. 416–425. doi:10.1093/ajcn/7.4.416.
David, S. et al. (2022) ‘Dysregulation of iron homeostasis in the central nervous system and the role of ferroptosis in Neurodegenerative Disorders’, Antioxidants & Redox Signaling, 37(1–3), pp. 150–170. doi:10.1089/ars.2021.0218.
David, S., Ryan, F., et al. (2022) ‘Ferroptosis in neurological disease’, The Neuroscientist, 29(5), pp. 591–615. doi:10.1177/10738584221100183.
Omena, J. et al. (2021) ‘The effect of food and nutrients on iron overload: What do we know so far?’, European Journal of Clinical Nutrition, 75(12), pp. 1771–1780. doi:10.1038/s41430-021-00887-5.
Kumar, A. et al. (2022) ‘Iron deficiency anaemia: Pathophysiology, assessment, Practical Management’, BMJ Open Gastroenterology, 9(1). doi:10.1136/bmjgast-2021-000759.
Hower, V. et al. (2009) ‘A general map of iron metabolism and tissue-specific subnetworks’, Molecular BioSystems, 5(5), p. 422. doi:10.1039/b816714c.
Piperno, A., Pelucchi, S. and Mariani, R. (2020) ‘Inherited iron overload disorders’, Translational Gastroenterology and Hepatology, 5, pp. 25–25. doi:10.21037/tgh.2019.11.15.
Seyoum, Y., Baye, K. and Humblot, C. (2021) ‘Iron homeostasis in host and gut bacteria – a complex interrelationship’, Gut Microbes, 13(1). doi:10.1080/19490976.2021.1874855.
Li, J. et al. (2020) ‘Ferroptosis: Past, present and future’, Cell Death & Disease, 11(2). doi:10.1038/s41419-020-2298-2.
Snyder, A.M. and Connor, J.R. (2009) ‘Iron, the substantia nigra and related neurological disorders’, Biochimica et Biophysica Acta (BBA) - General Subjects, 1790(7), pp. 606–614. doi:10.1016/j.bbagen.2008.08.005.
Laduron, P. (1982) ‘Brain dopamine receptor: Multiple binding sites or physiological receptor site’, Advances in Dopamine Research, pp. 71–82. doi:10.1016/b978-0-08-027391-4.50010-1.
Blatt, S.L. (2022) ‘Evaluation of anemia in thyroid dysfunctions anemia in thyroid dysfunctions: Retrospective cross-sectional study’, Clinical Pathology & Research Journal, 6(1), pp. 1–12. doi:10.23880/cprj-16000149.
Cempaka, A.R. et al. (2019) ‘Dysregulated iron metabolism-associated dietary pattern predicts an altered body composition and metabolic syndrome’, Nutrients, 11(11), p. 2733. doi:10.3390/nu11112733.